If you have ever watched a speech-language pathologist ask a child to stick out their tongue, wiggle it side to side, and then say “pa-ta-ka” as fast as they can, you have seen part of an oral mechanism exam without realizing it. From the outside, it looks like a simple game. On the inside, there is a massive amount of clinical mapping going on.
This assessment—frequently called an oral peripheral examination or an oral-facial examination—is one of the very first things an SLP does. Before diagnosing a speech sound disorder, starting articulation therapy, or looking into a swallowing issue, you have to look at the physical tools the person is working with. The oral mechanism exam is not some optional box to tick off. It is the core clinical foundation that decides the direction of everything you do next.
This guide will walk you through what the exam actually is, exactly what SLPs are searching for, how it plays out step by step, and what the results mean. We will also break down how the process shifts when you are working with kids versus adults, and what ASHA has to say about it. Whether you are a graduate student prepping for your very first clinic placement, a parent trying to make sense of a new referral, or a practicing SLP wanting a clean refresher, this guide has you covered.
What Is an Oral Mechanism Exam?
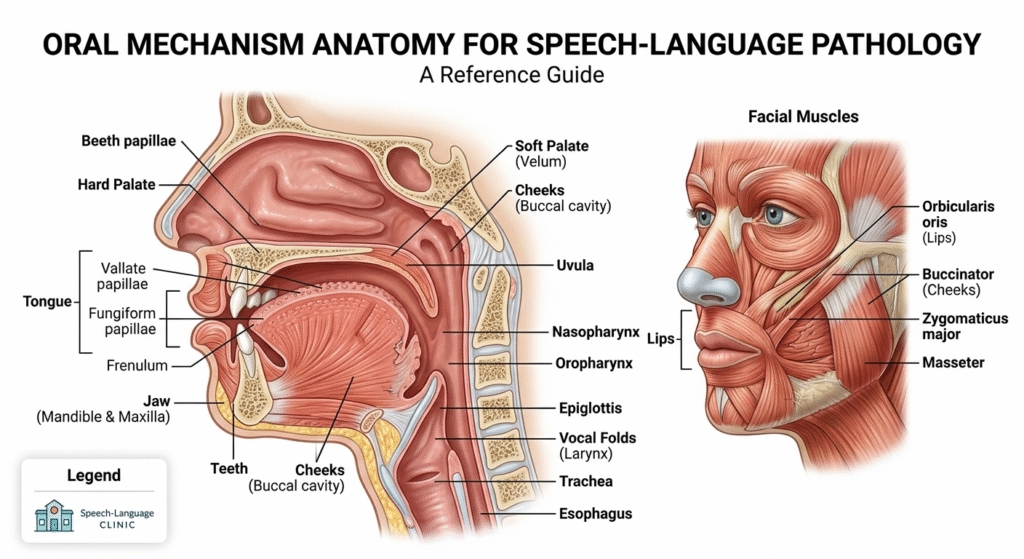
An oral mechanism exam is a hands-on clinical look at the physical structures and real-time muscle movements we use to talk and swallow. We are talking about the lips, tongue, jaw, hard palate, soft palate, teeth, cheeks, uvula, and overall facial muscles. The SLP tests every single one of these areas for two key things: structure (what it looks like when nothing is moving) and function (how well it actually works when the patient tries to move or speak).
The main thing the examiner wants to figure out is simple: Is a physical issue inside the mouth or a muscle control problem causing or adding to the communication or feeding trouble?
Think about it this way. A child who cannot get the /r/ sound right might have a tight lingual frenulum physically anchoring their tongue to the floor of the mouth. An adult who just had a stroke might have one-sided tongue weakness that makes their words sound slurred. Or someone with a very nasal voice might have a soft palate that fails to close off the airway to the nose. You cannot spot any of these underlying issues without an upfront, physical check of the oral mechanism.
For speech-language pathologists, this exam is a completely standard piece of a full speech and language evaluation. The entire thing takes just 10 to 20 minutes. Of course, that timeframe fluctuates depending on how complex the medical history is and how willing the patient is to cooperate—which is always an adventure when you have a toddler in the clinic chair.
Why the Oral Mechanism Exam Matters Clinically
The oral mechanism exam changes how a patient’s therapy path unfolds. It saves weeks, sometimes months, of mismatched treatment by pointing out the root cause of a speech or swallowing struggle.
Let’s look at an everyday example. Say an SLP is working with a kid who leaves out or mixes up a lot of speech sounds. It is easy to guess the child has a phonological disorder, which is a brain-based pattern issue rather than a muscle issue. But if the oral mechanism exam reveals an exceptionally high, narrow palate and minimal tongue movement, that guess goes out the window. Classic phonological therapy will not fix a physical space issue in the mouth.
On the adult side, a patient might come in complaining of a scratchy voice change or mild choking when drinking water. If the SLP notices a major droop or weakness on one side of the soft palate during the physical exam, it raises a flag for neurological changes. That finding tells the clinician to get the patient to a neurologist for a medical workup before speech therapy even starts.
At the end of the day, the exam determines whether a speech or swallowing issue comes down to:
- Structural Abnormalities: True differences in the physical shape, size, or wholeness of the mouth parts.
- Neuromuscular Dysfunction: Cases where the mouth parts look entirely normal at rest, but the nerves and muscles fail to move them properly.
Making this distinction is everything when it comes to an accurate differential diagnosis. On top of that, it gives you a solid baseline. Knowing precisely what a client can and cannot do with their articulators on day one gives the SLP concrete data points to track over time to see if therapy is actually working.
What the Oral Mechanism Exam Evaluates: Structure by Structure
Facial Symmetry and Muscle Tone
The SLP begins by quietly watching the patient’s face at rest before giving a single instruction. They are checking to see if both sides of the face look balanced, noting if the muscles seem overly stiff or unusually loose, and scanning for tiny, involuntary muscle ripples or twitches.
After that, the patient gets asked to do a few basic facial movements: smile wide, pucker up like they are blowing a kiss, puff out their cheeks with air, and lift up their eyebrows. This simple sequence shows whether the facial nerves are communicating with the muscles properly. If a face looks perfectly level at rest but drops completely on one side during a smile, that is a huge clinical clue. Weakness on just the bottom half of one side of the face usually hints at an upper motor neuron issue, while a drop that shuts down the whole side of the face—including the forehead—typically means a lower motor neuron problem.
Lips
The lips are absolutely essential for a massive chunk of our speech sounds. Sounds like /p/, /b/, and /m/ require the lips to seal shut completely to build up air. Sounds like /f/ and /v/ need the lower lip to press cleanly against the upper teeth. Any weakness or stiffness here shows up immediately in blurred speech.
The clinician looks over the lips for unusual shape variations, scarring, or asymmetry. To test movement, they have the patient pucker, smile, and rapidly swap back and forth between the two profiles. To check muscle strength, the SLP might have the patient squeeze their lips tight around a clean tongue depressor while the examiner gives it a gentle tug outward.
Jaw
When checking out the jaw, the SLP looks at where it sits at rest, how wide the patient can open it, and whether it moves in a straight line. If the jaw slides or veers off to one side when opening wide, it often signals a muscle weakness on that side or an issue with the temporomandibular joint.
The patient is asked to open wide, close, slide the jaw left and right, and push the bottom teeth forward. The clinician writes down any restricted movement, clicking or grinding sounds, or complaints of pain. Because the jaw acts as the steady foundation that the lips and tongue jump off from to speak or chew, an unstable jaw can mess with speech and eating in unexpected ways.
Teeth and Dental Alignment
SLPs do not care about teeth for dental health reasons; they care about how the setup of the teeth impacts speech sounds. Gaps from missing front teeth completely alter how air moves through the mouth, which frequently creates a noticeable lisp on sounds like /s/ and /z/. Structural bites, like an open bite where the front teeth fail to meet even when the back teeth touch, make it tough to stop air from leaking out on those same sounds.
The clinician looks for overbites, underbites, crossbites, and massive crowding. For older adults, checking how securely their dentures sit is vital, because loose or poorly fitting plates alter articulation and swallowing habits dramatically.
Tongue

The tongue is the powerhouse of speech production, so it gets the lion’s share of attention during the oral mechanism exam. The SLP views it from multiple angles and puts it through a series of movement challenges.
While the tongue rests on the floor of the mouth, the examiner checks its overall size relative to the rest of the cavity. A massive tongue can crowd things and muffle clarity. They also look for fasciculations, which are tiny, worm-like muscle twitches that can mean lower motor neuron trouble.
Then come the movement tasks. The patient sticks their tongue straight out, lifts the tip up to the bumpy ridge right behind the front teeth, drops it down toward the chin, and clears it side to side into the corners of the mouth. The SLP grades these actions based on speed, range, symmetry, and strength. Finally, they check the lingual frenulum underneath. If that little tissue string is too short or tight—often called a tongue-tie—it tethers the tongue down and stops the tip from hitting the roof of the mouth for sounds like /l/, /t/, and /d/.
Hard Palate
The hard palate is the bony ceiling of the front half of the mouth. Using a small penlight, the SLP checks its color, shape, and structure.
A ceiling that is unusually high and arched tightens the physical workspace the tongue has to move in, which often forces patients to push their sounds too far back in the mouth. A classic cleft palate is obvious right away, but a hidden submucous cleft takes a sharper eye. The examiner looks for a thin, faint bluish line down the center of the roof, a split uvula, or a small physical notch at the very back edge of the hard bone.
Soft Palate and Uvula
The soft palate, or velum, and the uvula hang out at the back of the mouth. To check them, the patient opens wide and holds a long “ah” sound.
For normal speech, the soft palate needs to lift up and pull backward to touch the back wall of the throat. This action shuts down the pathway to the nose, ensuring air only exits through the mouth during oral sounds. If that seal is incomplete or lazy, air escapes through the nose, making the voice sound hypernasal. The exam checks to see if the palate lifts evenly on both sides; a lazy lift on one side usually points to nerve weakness on that side. A split uvula is also tracked closely, as it often pairs with hidden palate variations.
Pharynx and Tonsils
The clinician takes a quick peek past the soft palate into the throat area to look at tissue color and the size of the tonsils. Heavily enlarged or swollen tonsils can physically crowd the back of the mouth, causing a muffled voice quality or stopping the soft palate from closing all the way, which skews speech resonance.
How to Do an Oral Mechanism Exam: Step-by-Step Clinical Workflow
Step 1: Pre-Exam Observation
The exam actually starts before the formal testing begins. While talking casually in the waiting area or watching a kid interact with toys, the SLP gathers real-world data. How does the jaw look at rest? Is there any drooling or poor saliva control? Does the face move evenly during an authentic laugh? These relaxed observations tell the clinician which areas need the closest focus during the structured steps.
Step 2: Structural Inspection
Next, the clinician moves systematically from the outside in. Using a penlight, a tongue depressor, and occasionally a small mirror to show the patient what to do, the SLP inspects the face, lips, jaw, teeth, tongue, hard palate, soft palate, and throat. Every single piece of structural data is written down on an assessment checklist or digital chart.
Step 3: Non-Speech Motor Tasks
The SLP then asks the patient to move individual mouth parts without making a sound. This separates physical muscle control from the mental work of talking. It is surprisingly common for a child to say a sound perfectly in a word but struggle to move that exact same muscle on command outside of speech. That contrast gives the clinician highly valuable diagnostic clues.
Standard movement tasks include:
- Lips: “Smile as big as you can,” “Pucker your lips like you are blowing out a candle,” and “Hold your lips shut tight.”
- Tongue: “Stick your tongue straight out,” “Try to touch your nose with your tongue tip,” and “Push your tongue into the side of your cheek.”
- Jaw: “Open your mouth as wide as possible” and “Slide your jaw side to side.”
- Soft Palate: “Open wide and say ‘ah, ah, ah’.”
Step 4: Diadochokinetic Tasks (DDK)
Diadochokinesis sounds complex, but it simply means testing how fast and smoothly a person can alternate between rapid movements. In this exam, that means repeating specific syllable lines to stress-test separate parts of the mouth.
First, the clinician tests Alternating Motion Rates using three basic syllables:
- “pa-pa-pa”: Tests how quickly and cleanly the lips open and close.
- “ta-ta-ta”: Tests the agility of the front tip of the tongue against the roof of the mouth.
- “ka-ka-ka”: Tests the speed of the back of the tongue hitting the soft palate.
The SLP counts how many times the patient can repeat the syllable per second, listening for a steady, even rhythm and clear sound production.
Next, they test the Sequential Motion Rate by combining the sounds: “pa-ta-ka” (or “patty-cake” for young kids). This forces the brain and mouth to cycle rapidly through three separate movement spaces: front, middle, and back. If a patient handles the single sounds perfectly but scrambles or falls apart on “pa-ta-ka,” it generally points to a speech motor planning issue like apraxia, rather than simple muscle weakness.
Step 5: Connected Speech and Swallowing Observation
To wrap things up, the clinician watches how all these moving pieces function together during natural conversation, reading out loud, or storytelling. They look to see if the physical hurdles spotted during the isolated movement steps actually show up to disrupt everyday speech.
If the patient has feeding or swallowing concerns, the SLP adds a brief, informal swallow screening. They watch the patient take a sip of water or swallow their own saliva, tracking the timing, watching for a smooth lift of the throat, and listening closely for any coughing, throat clearing, or a wet, gurgly voice after the swallow.
Conditions Identified During an Oral Mechanism Exam
While the oral mechanism exam is rarely used to diagnose a medical condition completely on its own, its findings provide the foundational proof that points toward the right diagnosis.
- Dysarthria: This neurological speech disorder weakens the muscles used for talking. Common exam findings include poor tongue strength, asymmetrical lip movement, muscles that feel either rigidly tight or completely floppy, and slow, dragging DDK rates. This condition is frequently caused by a stroke, traumatic brain injury, Parkinson’s disease, or ALS.
- Childhood Apraxia of Speech (CAS): Children with CAS often display perfectly normal physical oral structures and full muscle strength when doing simple tasks. However, their speech errors are highly inconsistent, and they struggle immensely with the rapid coordination needed for the “pa-ta-ka” sequence. This contrast between strong muscles and poor movement coordination is a classic diagnostic hallmark.
- Cleft Palate and Velopharyngeal Dysfunction (VPD): Visible gaps or poor upward movement of the soft palate point directly to VPD. This allows air to escape through the nose, resulting in a hypernasal voice and a tough time building up enough air pressure in the mouth to say crisp sounds like /p/, /t/, or /s/.
- Ankyloglossia (Tongue-Tie): This is identified when visual inspection shows an unusually short, tight string under the tongue that visibly holds the tongue tip down or causes it to heart-shape when pushed forward.
- Parkinson’s Disease: During an evaluation, individuals with Parkinson’s often present with a reduction in facial expressions, minimal lip movement while talking, a quiet voice, and a rapid, trailing off, or highly hesitant DDK rate.
Pediatric vs. Adult Oral Mechanism Exams: Key Differences
Pediatric Evaluations
Testing a young child requires flexibility, speed, and creativity. A toddler will not sit perfectly still and stick out their tongue on command. Experienced pediatric SLPs turn the entire evaluation into a game. They might use flavored tongue depressors as “dinosaur teeth checkers,” look in a mirror together to make funny faces, or practice making silly animal sounds to sneakily check muscle function.
Age and development matter immensely when interpreting the results. A slight tongue-thrust or forward resting position is perfectly normal for a two-year-old but stands out as a true clinical concern in a seven-year-old. Clinicians always compare a child’s movements against developmental growth charts, not adult standards. Gathering a thorough feeding history is also critical, as early struggles with nursing, transitioning to solid foods, or avoiding specific textures often trace back to the same motor deficits causing their speech delays.
Adult Evaluations
Working with adults is much more straightforward instruction-wise, but analyzing the results can be highly complex—especially when dealing with aging or progressive neurological conditions.
Special care must be paid to dental appliances. It is ideal to check a patient’s mouth both with their dentures in and with them removed. Poorly fitting dentures can wreck a person’s articulation and make swallowing dangerous, and many adults develop major, unnatural speech habits just to keep loose dentures from slipping out of place.
The natural aging process also changes oral motor function. Older adults naturally experience a slight drop in tongue strength, a slower overall speech rate, and milder loss of muscle elasticity. The evaluating SLP must use careful interviewing and standardized data to separate expected, healthy aging from a true underlying neurological disease.
For individuals dealing with progressive conditions like ALS or Multiple Sclerosis, these initial structural exams act as a vital baseline. Regular follow-ups allow the healthcare team to track changes over time and introduce proactive communication tools.
ASHA Guidelines and Evidence-Based Practice
The American Speech-Language-Hearing Association (ASHA) firmly establishes the oral mechanism examination as an absolute requirement for any comprehensive speech, language, or swallowing assessment. It is officially built into the professional scope of practice across all clinical settings.
ASHA does not force clinicians to use one single, mandated PDF form or checklist. Instead, they expect the SLP to use their own clinical judgment to alter the focus of the exam based on why the patient is seeking care. However, ASHA strongly emphasizes that all observations must be tracked and documented systematically to build reliable, evidence-based treatment plans.
Clinicians looking for standardized, norm-referenced comparisons often turn to formal assessment kits like the Oral Speech Mechanism Screening Examination (OSMSE-3) or the Frenchay Dysarthria Assessment. Most university training programs design their own highly detailed templates—such as the widely used Lamar University Oral-Facial Examination Form—to ensure graduate students learn to evaluate every single structural and motor category thoroughly. For clinicians seeking current, evidence-based resources on comprehensive speech evaluation including oral mechanism examination, ASHA’s Practice Portal provides regularly updated clinical guidance. The American Academy of Neurology clinical guidelines cover neurological evaluation protocols relevant to motor speech assessment in neurological populations.
Common Abnormal Findings and What They Suggest
To help visualize how structural checks connect to clinical issues, it can be useful to look at common red flags and their meanings side by side.
| Observation / Finding | What It Looks Like Physically | What It Often Suggests Clinically |
| Tongue Deviation | The tongue tips sharply to one side when pushed out. | Weakness on the side it points toward; points to Hypoglossal Nerve (CN XII) damage. |
| Asymmetrical Smile | One side of the mouth smiles normally; the other side stays flat or drops. | Facial Nerve (CN VII) weakness; common after a stroke or in Bell’s Palsy cases. |
| Hypernasality | Explicit nasal air leakage during vowels and pressure sounds. | Incomplete velopharyngeal closure due to structural clefts or weak palate muscles. |
| Irregular SMR Rhythm | The patient scrambles or breaks down trying to say “pa-ta-ka.” | Difficulty with motor planning and sequencing, highly typical of Apraxia. |
| Lingual Fasciculations | The tongue looks like a “bag of worms” with tiny, constant muscle ripples at rest. | Lower motor neuron degeneration; frequently monitored in conditions like ALS. |
Do SLPs Always Have to Do an Oral Mechanism Exam?
This question pops up constantly among busy clinicians and students facing tight schedules. The direct answer is yes: professional standards position it as an indispensable part of a new evaluation. Skipping this step means missing the physical context of the communication struggle.
In the real world, an experienced school-based SLP who has worked with a child for years might perform a quick, informal check rather than a massive 20-minute formal exam when re-evaluating for an IEP. However, for any fresh evaluation, any case involving motor speech concerns, any swallowing referral, or any complex case where diagnostic clarity is muddy, the oral mechanism exam cannot be skipped.
Skipping this step is a lot like trying to read the final conclusion of a medical report without looking at the lab work that led there—the final guess might end up being right, but you lack the structural proof to back it up.
A thorough assessment acts as the anchor for all downstream treatment. To understand this workflow better, you can see parallels in our article detailing The CPA Exam Failure Journey, which looks closely at how missing foundational diagnostic reviews can derail long-term professional milestones. Similarly, just as a medical provider relies on an Eye Exam to structurally isolate vision issues from cognitive ones, keeping a sharp eye on physical oral baselines ensures a patient is set up for true long-term success.
Frequently Asked Questions
What is an oral mechanism exam?
It is a structured clinical checkup performed by an SLP to examine the physical structures and movement patterns used for speaking and swallowing. It checks the lips, tongue, jaw, teeth, palates, and facial muscles to see if structural differences or nerve/muscle issues are hurting communication skills.
What is the main purpose of an oral mechanism exam?
The purpose is to discover whether a physical or neurological issue in the mouth is causing or worsening a speech or swallowing problem. It helps clinicians differentiate between structural, motor planning, and phonological issues so they can design the right therapy program.
How long does an oral mechanism exam take?
A standard, comprehensive exam takes between 10 and 20 minutes. It can take a bit longer if a patient has a complex neurological condition that requires detailed tracking, or if a clinician needs extra time to guide a young child through the steps.
Is an oral mechanism exam painful?
Not at all. The entire process is non-invasive and relies on simple visual tracking and basic movement requests. The SLP will use a smooth tongue depressor and a small light to look at the roof of the mouth, but nothing about the assessment causes pain.
What does an SLP look for during the exam?
The clinician evaluates physical structure, overall facial symmetry, resting muscle tone, range of movement, muscle strength, and the coordination and speed of rapid speech repetitions during specialized syllable drill tasks.
What is the oral mechanism exam PDF ASHA reference?
While ASHA doesn’t issue one specific official form for everyone to print out, they recognize standardized protocols like the OSMSE-3 and highly detailed university checklists, such as the Lamar University template, as gold-standard training guidelines.